Key Product Details
Assay Type
Solid Phase Sandwich ELISA
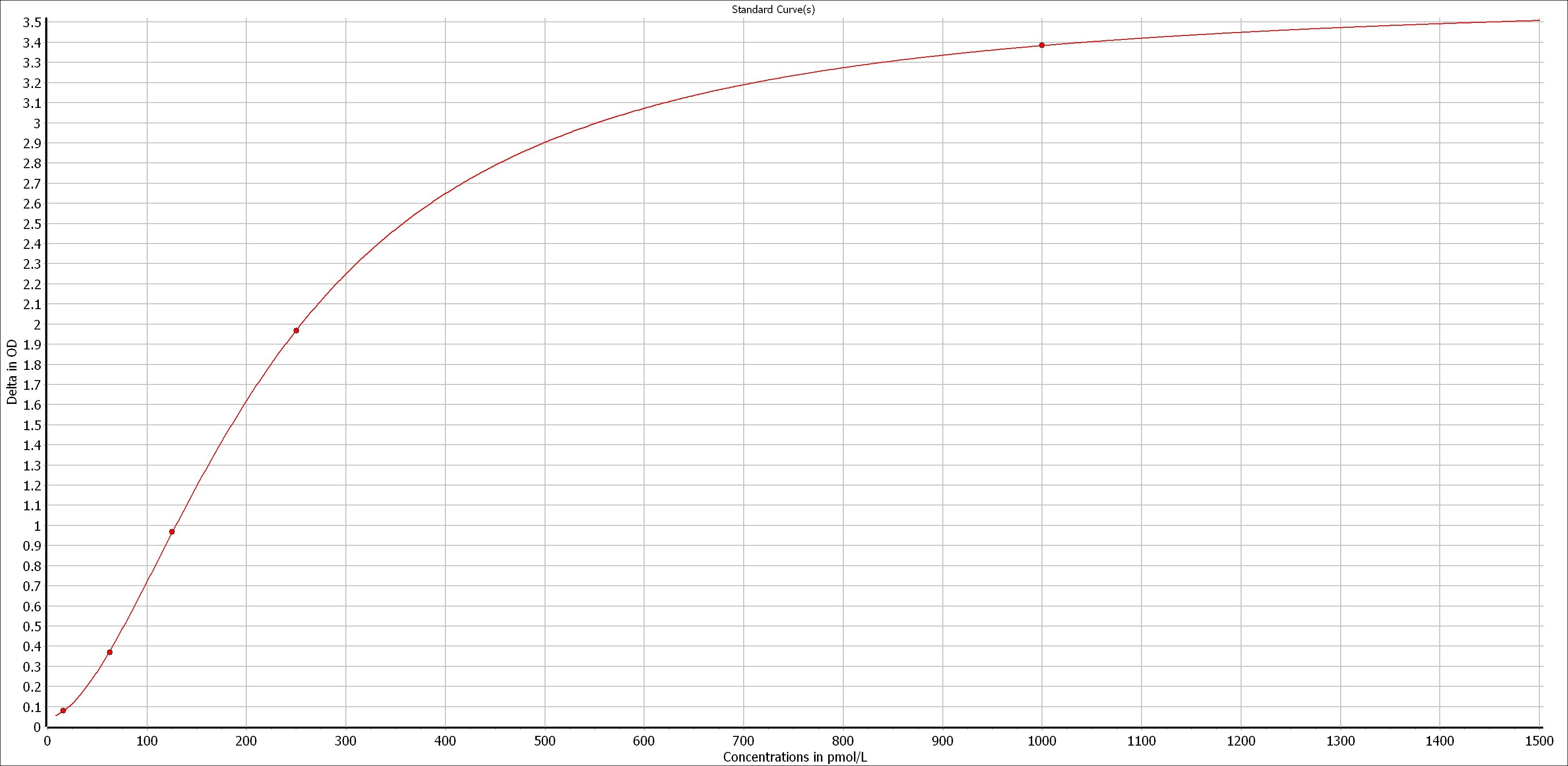
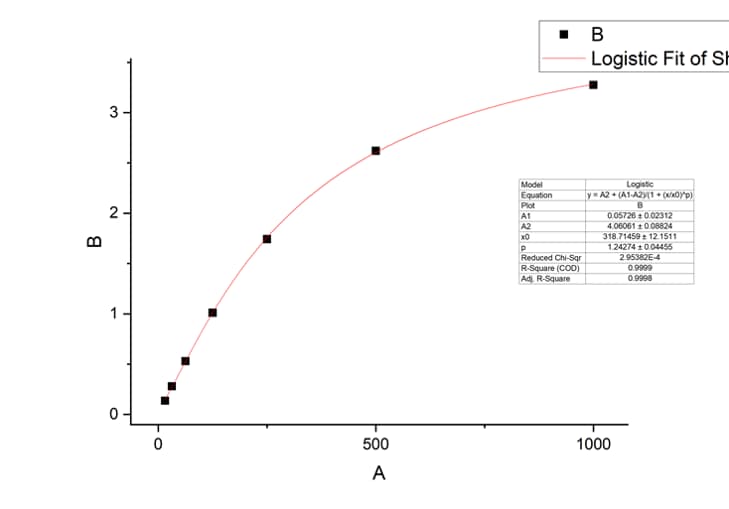
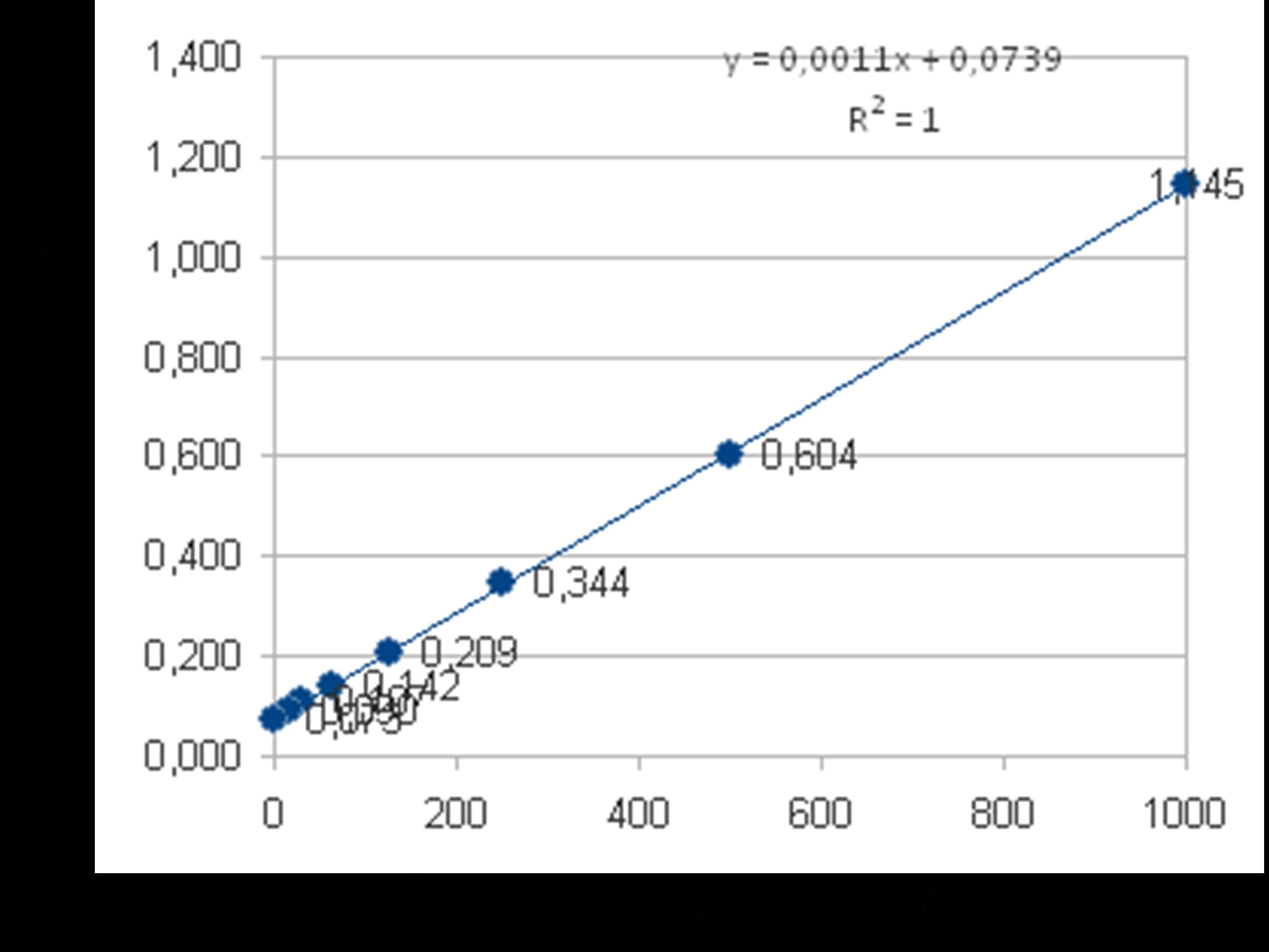
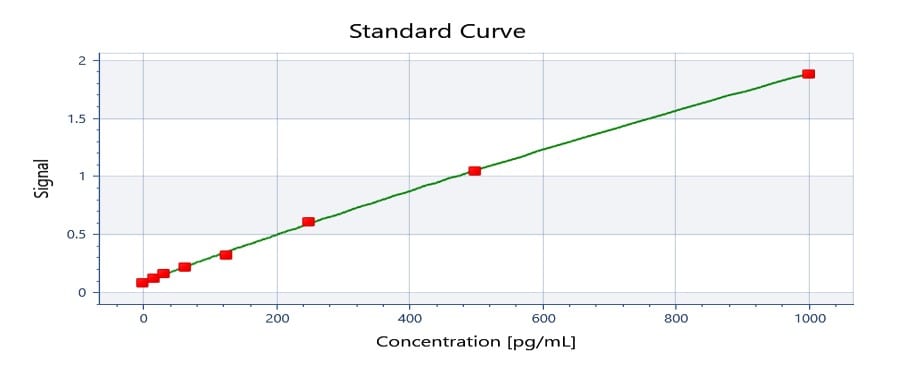
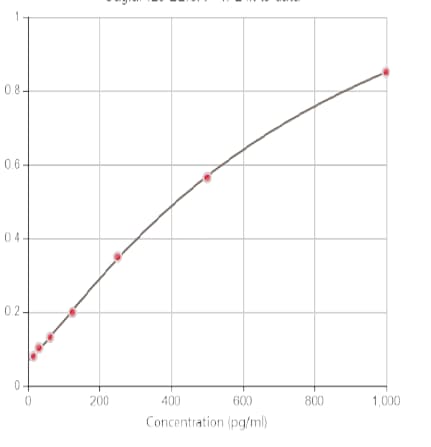
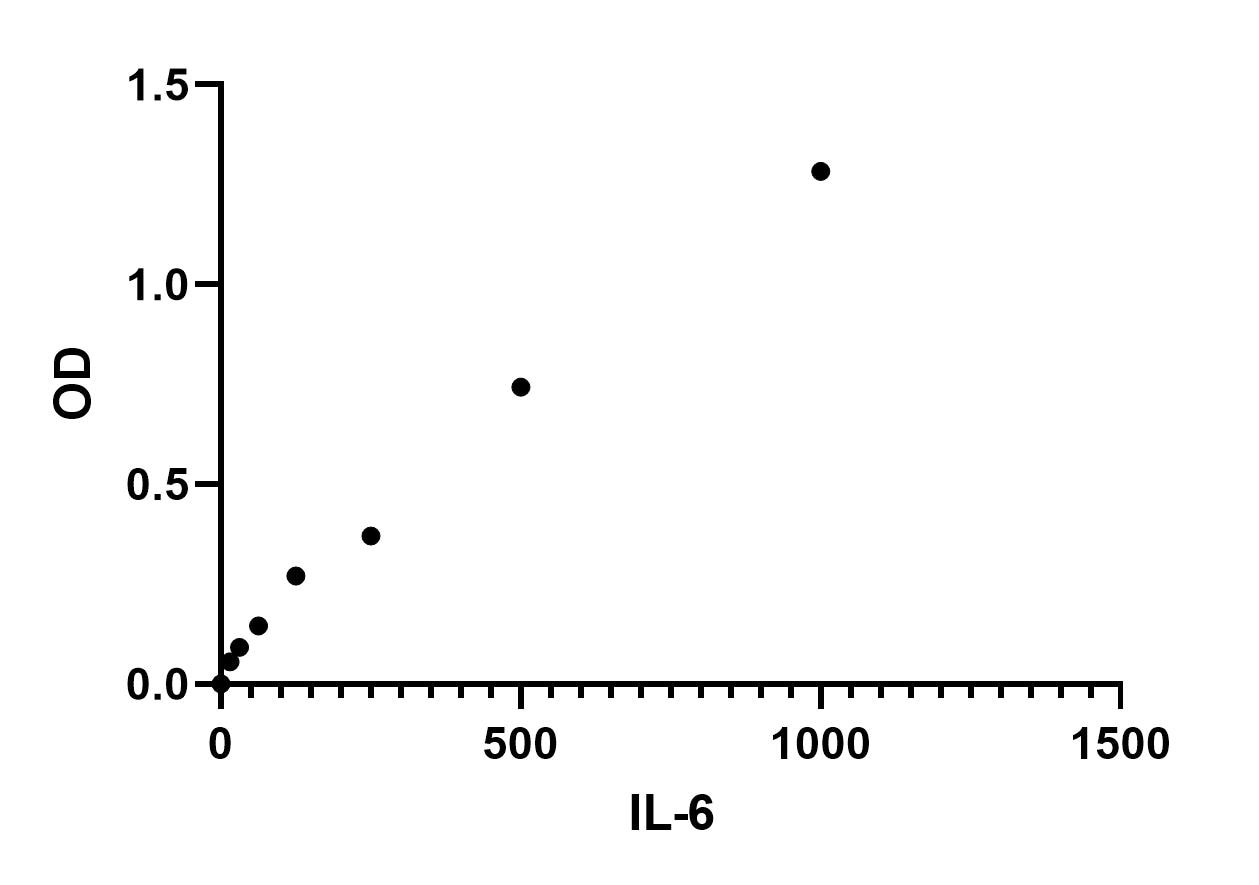
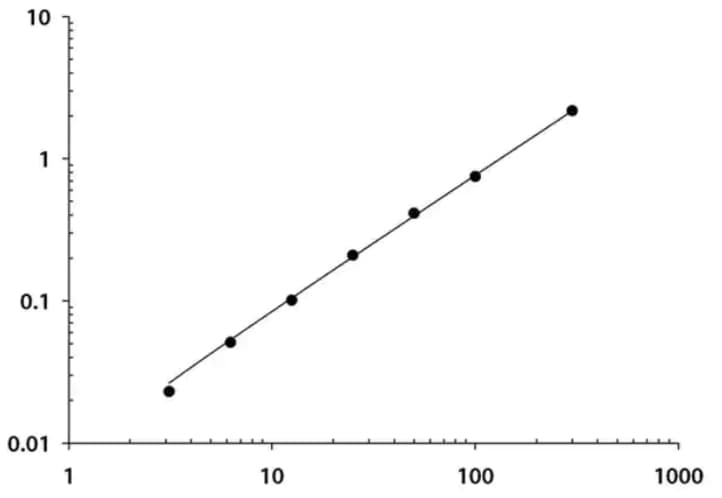
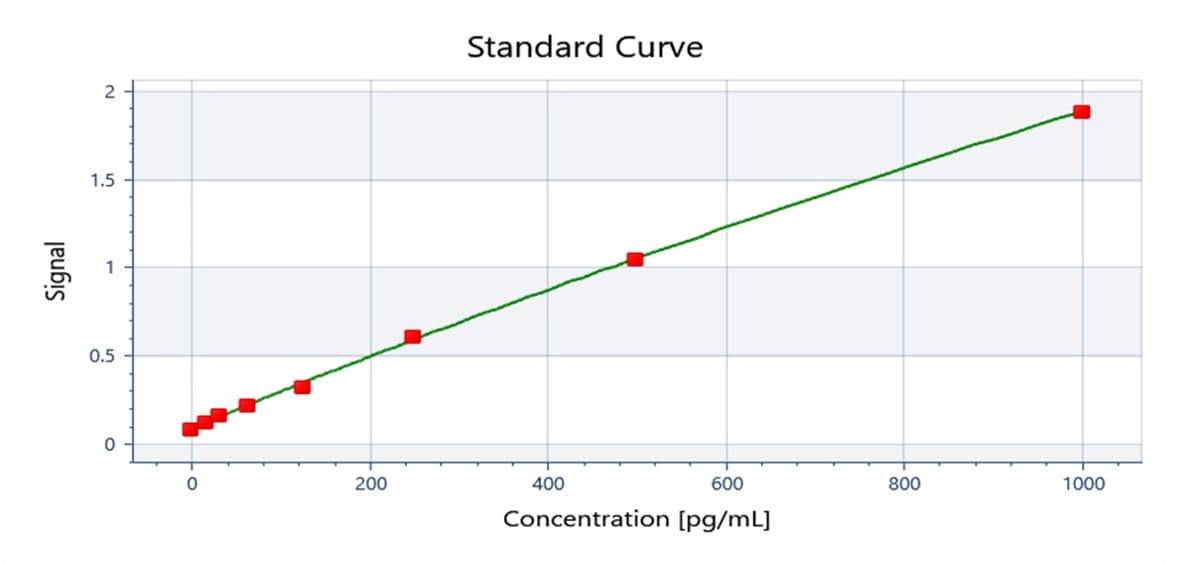
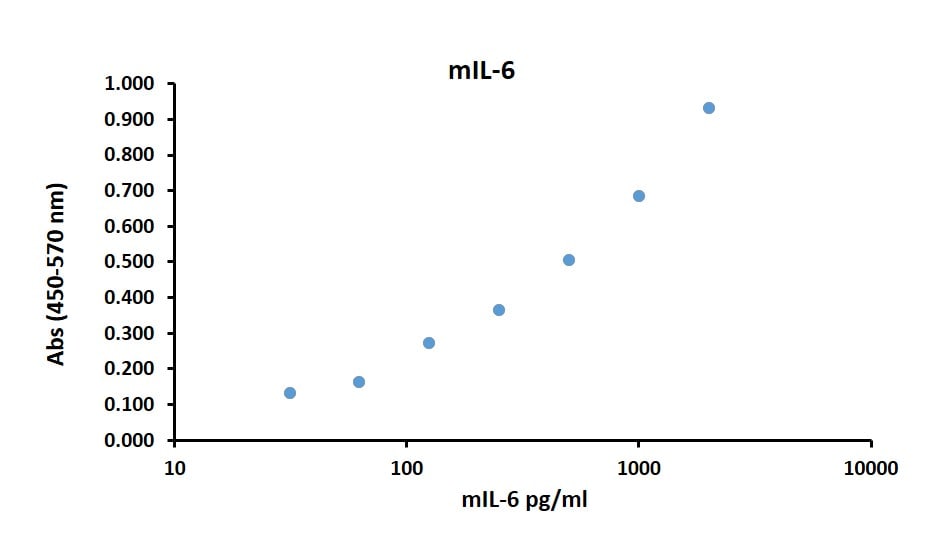
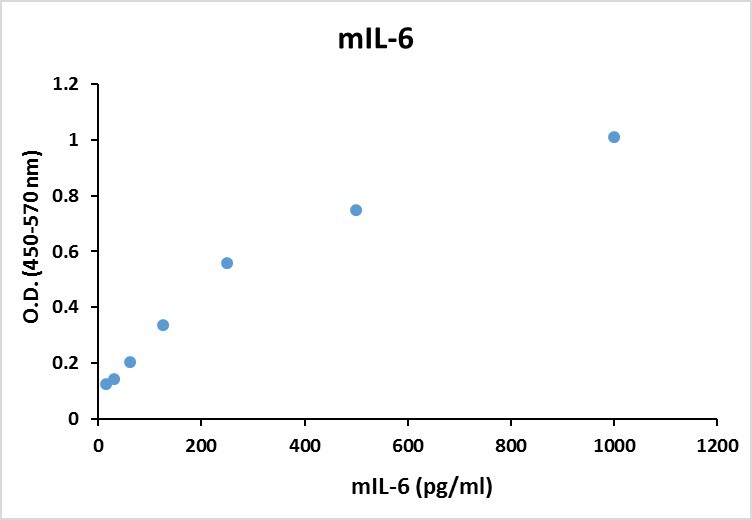
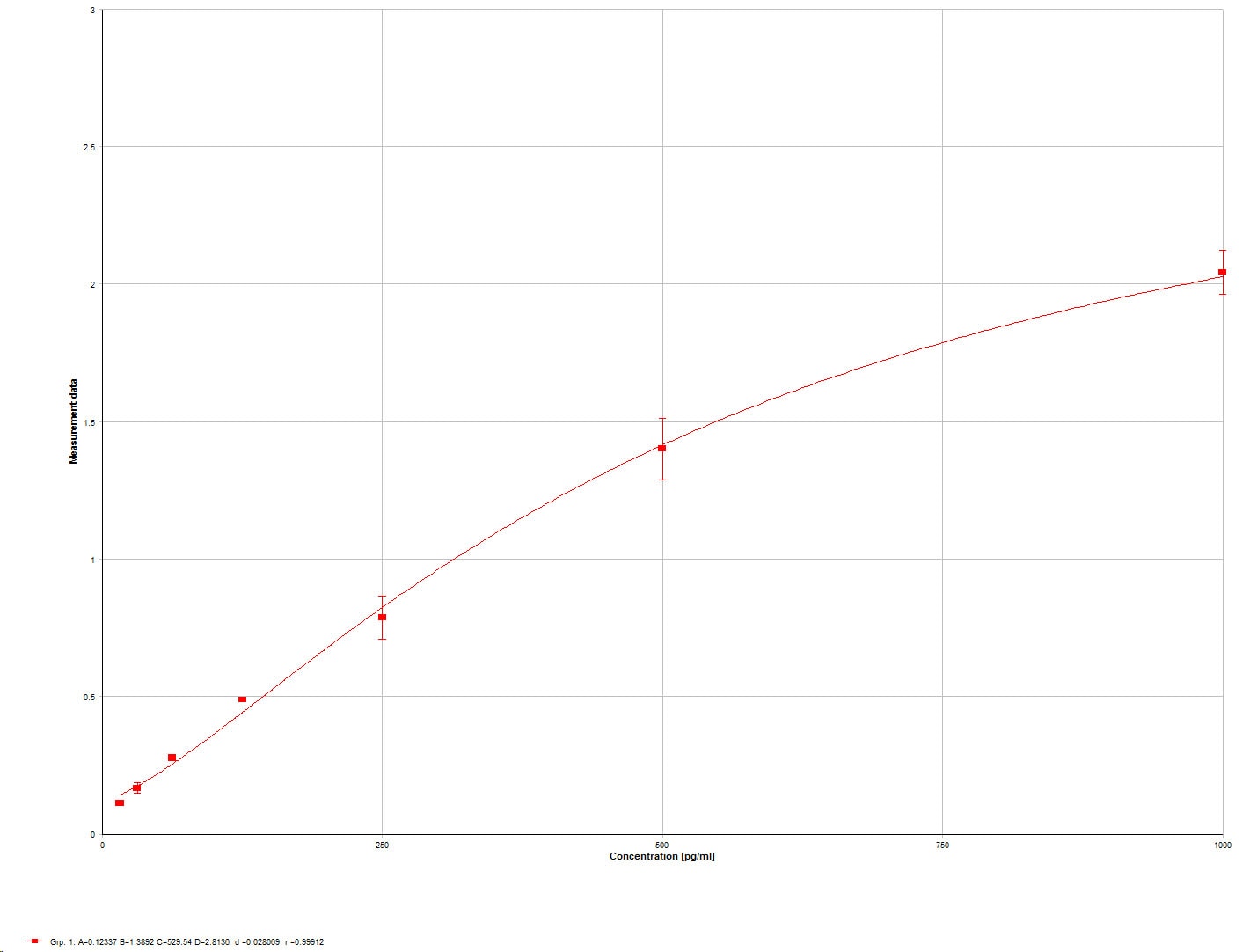
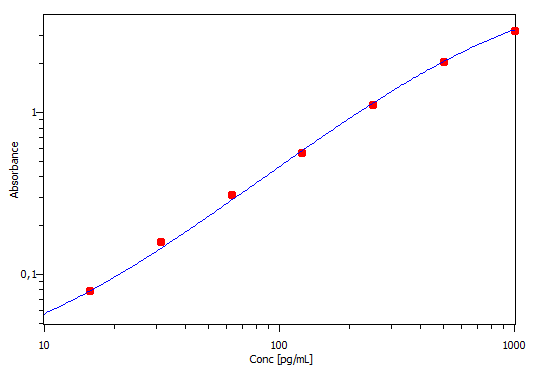
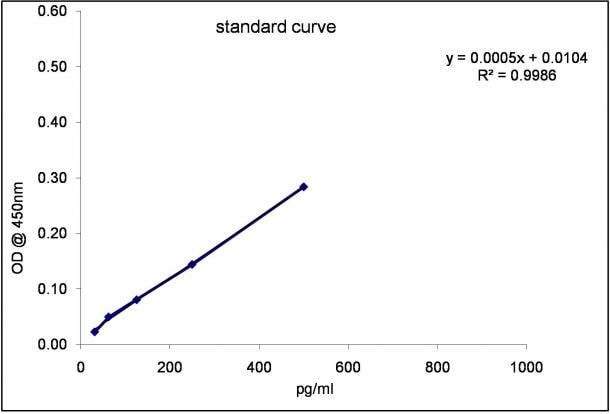
Assay Range
15.6-1000 pg/mL
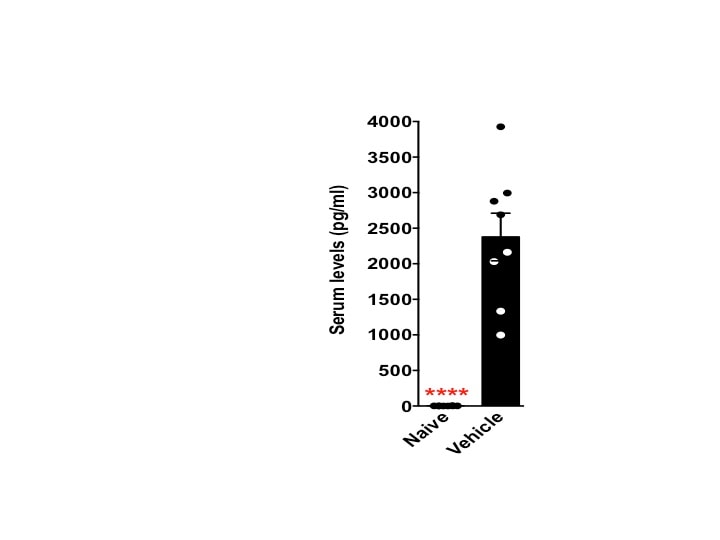
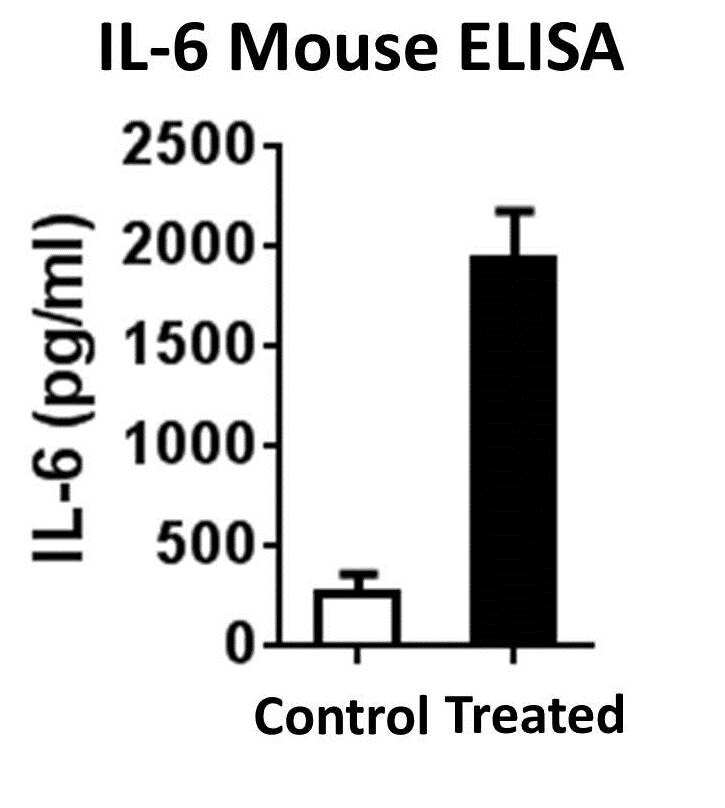
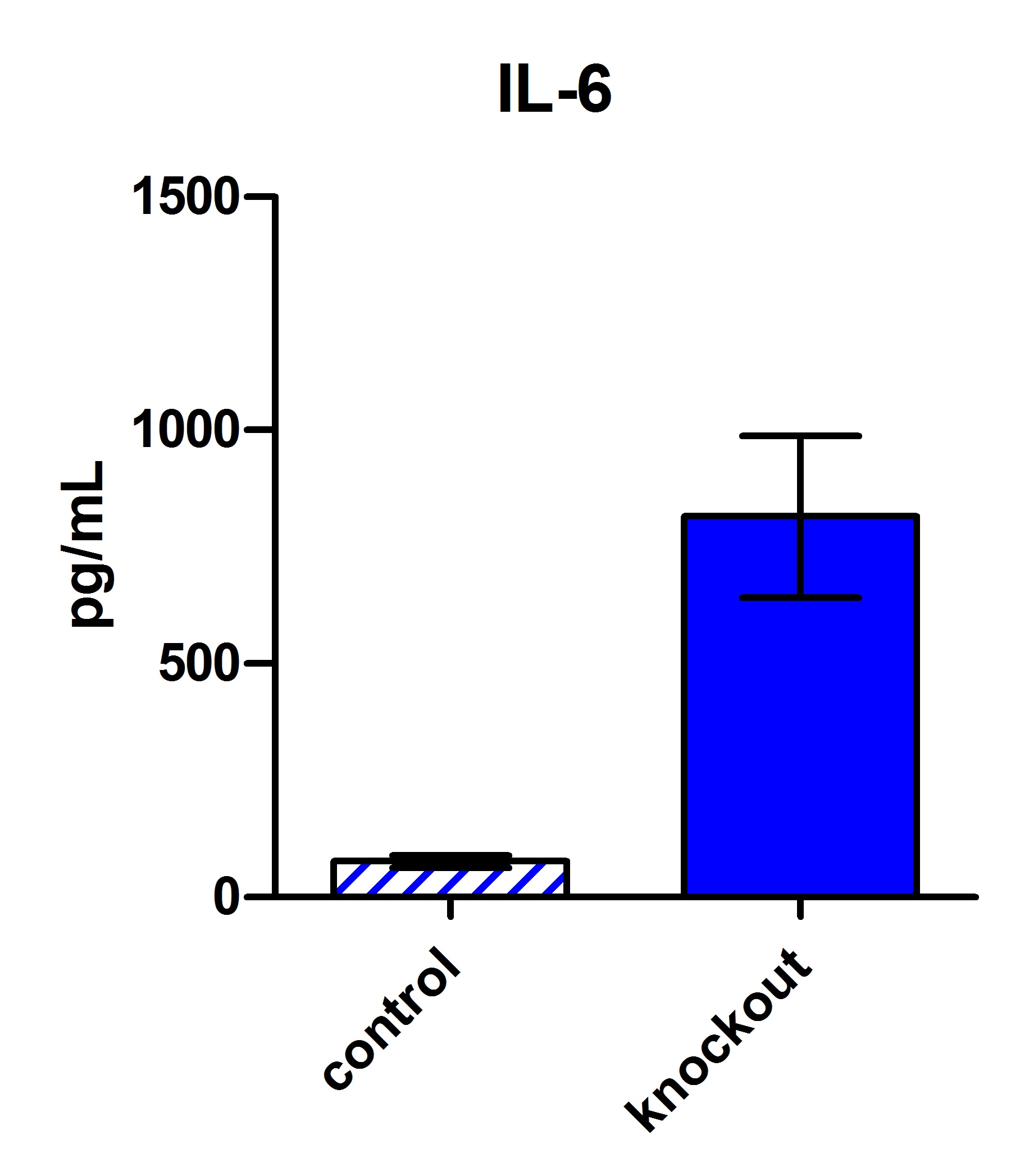
Sample Type
Cell culture supernates, serum, and plasma
Note: Diluents for complex matrices, such as serum and plasma, should be evaluated prior to use in this DuoSet
Mouse IL-6 DuoSet ELISA Features
- Optimized capture and detection antibody pairings with recommended concentrations save lengthy development time
- Development protocols are provided to guide further assay optimization
- Assay can be customized to your specific needs
- Economical alternative to complete kits
Other Reagents Required
DuoSet Ancillary Reagent Kit 2 (5 plates): (Catalog # DY008C) containing 96 well microplates, plate sealers, substrate solution, stop solution, plate coating buffer (PBS), wash buffer, and Reagent Diluent Concentrate 2.
PBS: (Catalog # DY006), or 137 mM NaCl, 2.7 mM KCl, 8.1 mM Na2HPO4, 1.5 mM KH2PO4, pH 7.2 - 7.4, 0.2 µm filtered
Wash Buffer: (Catalog # WA126), or equivalent
Reagent Diluent*
Blocking Buffer*
Substrate Solution: ELISA TMB Substrate (Catalog # DY999B or DY999B-250)
Stop Solution: Methanesulfonic acid (Catalog # DY994B or DY994B-250)
Microplates: (Catalog # DY990), or equivalent
Plate Sealers: (Catalog # DY992), or equivalent
*For the recommended Reagent Diluent and Blocking Buffer for a specific DuoSet ELISA Development Kit, refer to the product datasheet.
Background: IL-6
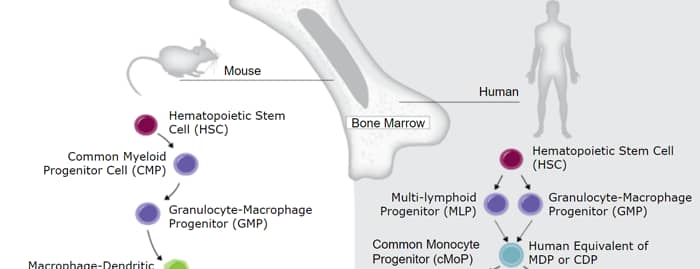
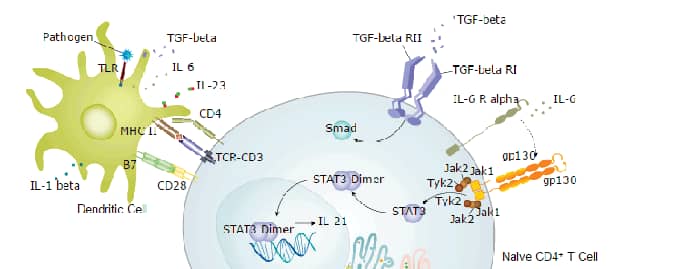
Interleukin 6 (IL-6) is a pleiotropic, a-helical, 22-28 kDa phosphorylated and variably glycosylated cytokine that plays important roles in the acute phase reaction, inflammation, hematopoiesis, bone metabolism, and cancer progression. Mature human IL-6 is 183 amino acids (aa) in length and shares 39% aa sequence identity with mouse and rat IL-6. Alternative splicing generates several isoforms with internal deletions, some of which exhibit antagonistic properties. Cells known to express IL-6 include CD8+ T cells, fibroblasts, synoviocytes, adipocytes, osteoblasts, megakaryocytes, endothelial cells (under the influence of endothelins), sympathetic neurons, cerebral cortex neurons, adrenal medulla chromaffin cells, retinal pigment cells, mast cells, keratinocytes, Langerhans cells, fetal and adult astrocytes, neutrophils, monocytes, eosinophils, colonic epithelial cells, B1 B cells and pancreatic islet beta cells. IL-6 production is generally correlated with cell activation and is normally kept in control by glucocorticoids, catecholamines, and secondary sex steroids. Normal human circulating IL-6 is in the 1 pg/mL range, with slight elevations during the menstrual cycle, modest elevations in certain cancers, and large elevations after surgery.IL-6 induces signaling through a cell surface heterodimeric receptor complex composed of a ligand binding subunit (IL-6 R alpha) and a signal transducing subunit (gp130). IL-6 binds to IL-6 Ra, triggering IL-6 Ra association with gp130 and gp130 dimerization. gp130 is also a component of the receptors for CLC, CNTF, CT-1, IL-11, IL-27, LIF, and OSM. Soluble forms of IL-6 Ra are generated by both alternative splicing and proteolytic cleavage. In a mechanism known as trans-signaling, complexes of soluble IL-6 and IL-6 Ra elicit responses from gp130-expressing cells that lack cell surface IL-6 Ra. Trans-signaling enables a wider range of cell types to respond to IL-6, as the expression of gp130 is ubiquitous, while that of IL-6 Ra is predominantly restricted to hepatocytes, monocytes, and resting lymphocytes. Soluble splice forms of gp130 block trans-signaling from IL-6/IL-6 Ra but not from other cytokines that use gp130 as a co-receptor.
IL-6, along with TNF-a and IL-1, drives the acute inflammatory response. IL-6 is almost solely responsible for fever and the acute phase response in the liver, and it is important in the transition from acute inflammation to either acquired immunity or chronic inflammatory disease. When dysregulated, it contributes to chronic inflammation in conditions such as obesity, insulin resistance, inflammatory bowel disease, arthritis, and sepsis. IL-6 modulates bone resorption and is a major effector of inflammatory joint destruction in rheumatoid arthritis through its promotion of Th17 cell development and activity. It contributes to atherosclerotic plaque development and destabilization as well as the development of inflammation-associated carcinogenesis.
Alternate Names
BSF-2, BSF2, IFNB2, IL6, MGI-2A
Additional IL-6 Products

 Powered by Bioz
Powered by Bioz